Medical Bits – Vol. 2.8: Your Health and Medical News
Our Brain
Our brain is the central organ of our Central Nervous System and it is connected to the spinal cord by the brainstem which harbors the midbrain, the pons and medulla oblongata. The midbrain is connected to the cerebellum by bilateral tracts. The brain is divided into 2 hemispheres and each hemisphere, conventionally divided into 4 lobes: frontal, temporal, parietal and occipital. Both hemispheres are similar in shape and function, but the left is preferentially responsible for language and the right for visual-spacial ability.
The first historical reference to the brain dates back to 1700 BC. An Egyptian battlefield surgeon describes in a papyrus two patients with compounded fractures of the skull and their symptoms, diagnosis, prognosis and recognizes the consequences of aphasia and convulsions. The Pythagorean Alcmaeon of Croton (6th to 5th centuries BC) was the first to consider the brain the seat of the mind and later Hippocrates, “the father of our scientific medicine” adopted this view and believed the brain to be the seat of Intelligence. Aristotle thought this belonged to the heart and hypothesized that the brain was in charge of “cooling” the blood. Later, during the Hellenistic period, additional observations by Herophilus and Erasistratus reaffirmed the central volitive role of the brain and its role in the control of muscles, which was accepted and expanded by Galen in the Roman Period. Much of this knowledge was “lost” in the European Middle Ages but preserved and expanded in the Islamic world through Avicennas, Averroes, Avenzoar, Maimonides and others. Finally, the rediscovery of the power of observation and experimentation during the Renaissance, led to deeper and more complete anatomic dissections by Andreas Vesalius and others which cemented the role of the brain and its dependent structures as the protagonist in charge of Intelligence and motor-sensory control.
Of course, any superficial discussion of “brain power” would be incomplete without a few words about the importance of neuroscience. Advances in molecular biology, electrophysiology, computer science, electronics, functional imaging, genetics and neuroscience in the last decades of the last millennium have enable us to learn how our brain works, develops, functions, malfunctions and how it can possibly be changed. But many mysteries remain. Some of the most conspicuous are the degenerative diseases of our central nervous system, such as Parkinson’s Disease, Dementia, Amyotrophic Lateral Sclerosis, Multiple Sclerosis and others.
At birth, the brain weighs 25% of an adult brain and contains 85-95 billion neurons. By age 2, its weight increases to 75% and by age 3 to 90% of an adult brain and by age 5 it has garnered most of its “computational power”. No wonder we should invest in pre-K education and ascertain a nurturing environment for our children.
This “growth” is due to the formation of synaptic connections and “myelinization” (deposit of insulating material around new “hard wiring”). Of course, we do not gain additional neurons as we grow, only additional synapses, more complex networks and neuronal “collaboration” fields.
The gray matter of the brain (which contains the neurons) matures from “back to front”. Maximum density of areas associated with sensory and motor tasks, is achieved in the occipital and temporo-parietal cortex in late childhood, but the proper maturation of the prefrontal cortex is reached in late adolescence and early adulthood.
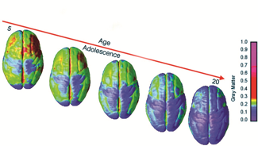
Higher cognitive functions such as assessing risks and behavioral control depend on this region of the brain. It should not be surprising that 65% of deaths among people ages 15-20 are due to traumatic or accidental injuries. The adolescent brain may have an “imbalance” that leads to excessive risk taking. It also explains why violent crime is mostly a vice of the young and quite rare after age 35 (and why criminal and penitentiary reforms are overdue).
Dementia
As you know, dementia is not a specific disease, but a general term that pertains to the progressive loss of cognitive functions of remembering, thinking and decision-making that impairs independence and performance of our activities of daily living. Some people just blame it on “old-age”, but cognitive dysfunction is not mandatory as we age. Mild cognitive impairment is an intermediate clinical state that can be a precursor but it may also be reversible (depression, trauma, medications, severe acute illness). Of course, the prevalence rises with aging. By age 70, 2% of humans have features of dementia and its incidence doubles every 5 years to the age of 90.
There are more than 50 million people worldwide living with dementia, and unfortunately, since longevity has increased, so has its prevalence. In 1920, life expectancy at birth was 35. Now it is over 80.
The most common conditions that cause dementia:
- Alzheimer Disease (accounts for 60-80%)
- Dementia with Lewy Bodies
- Frontotemporal dementia
- Parkinson’s disease dementia (accounts for 3-4% and more common as the disease progresses).
- Others: Vascular dementia, Progressive supranuclear palsy, multisystem atrophy, Cortico-basal degeneration, Huntington disease, HIV-related, Normal pressure hydrocephalus, Prion-related, Alcoholism-related and those due to mixed causes.
Most often family members are the first to pick up cognitive abnormalities.
Your physician may administer tests on attention, memory and problem solving. Physical exam, blood tests and brain scan should be completed. Of course, no one wants to “meet” Dr. Alois Alzheimer. While performing an autopsy in his native Germany, on August Deter in 1906, he noticed the brain of a 40-year-old “demented” patient had shrunk, many neurons had disappeared and there were abnormal plaques of knotty bundles of protein now called tau and beta-amyloid collecting between neurons.
Even allowing for their higher longevity, more than two-thirds of patients are women and the global prevalence of dementia is rising. The global cost of care was estimated at over $1trl in 2018 and may reach $2tril by 2030. It is estimated that as life expectancy rises, the cases will increase by 50% in the developed world and by more than 80% in poorer nations. Unfortunately, despite these “pandemic” proportions, dementia research is underfunded, in part because the mistaken public perception that it is part of aging (but a survey last year found 20% blamed “bad luck”, 10% “God’s will” and 2% “witchcraft”!). Another big part are the poor results after decades and multiple clinical trials. A paper reviewing clinical trials for Alzheimer’s drugs from 2002-2012 found a failure rate of 99.6%.
Four drugs have been approved for treatment, that tackle some of the symptoms but not the disease and have limited benefits with significant side-effects. So disappointing are the “benefits” of these Dementia drugs, that the French government stopped payment in 2018.
The problem may be that the slow accumulation of beta-amyloid plaques in the brain may develop 15 to 20 years before the onset of clinical disease. Surprisingly, a trial of anti-amyloid drug named Aducanumab was reported as negative in 2019 but another review of the same data indicated some benefits leading to FDA application for approval.
Oligomannate, derived from marine algae, was approved last year by China but Western researchers indicated the benefits were difficult to ascertain and (not surprisingly) data hard to discern.
Some genes have been associated with increased risk. The rise of a “tau” and amyloid protein in the cerebrospinal fluid may serve as markers and a new experimental blood test that measures p-tau217 offers hope and may identify Alzheimer’s with 95% accuracy.
What about herbs and nutritional supplements? A quick search on the subject yielded dozens of compounds purported to be beneficial to prevent memory loss or as “memory enhancers”. There are no supplements or remedies proven to be beneficial. Some have been formally studied, such as Ginkgo biloba with no beneficial effects. Phospholipids such as phosphatidylserine and phosphatidylcholine have been investigated with equivocal results. Fish oil, choline, B12, B6, selenium, nicotine and countless other chemical and micronutrients have been proposed and studied with negative results!
But after all this bleak information what can we do to avoid befriending Dr. Alzheimer?
A recent study estimated that dementia could be prevented or delayed in 40% of cases by avoiding head injuries, limiting excessive drinking, exposure to air pollution, controlling blood pressure, diabetes, obesity, treating hearing loss and eliminating smoking! And mindfulness training may give you peace, enjoyment and another edge to fight off Dementia, as discussed here: https://scholar.harvard.edu/sara_lazar/home
MEDICAL NEWS:
SARS-CoV2 Vaccine Development
I encourage you to read more about the subject in this interactive feature from the NYT that is updated frequently:
https://www.nytimes.com/interactive/2020/science/coronavirus-vaccine-tracker.html
As summarized by the Coronavirus Vaccine Tracker, there are now more than 137 vaccines in development with 11 in phase III, 14 in phase II and 27 in phase I clinical trials. There is one vaccine developed by CanSinoBIO, a Chinese company funded by the government and co-developed with the Chinese military, that has been approved for administration to the military (not known if mandatory or optional).
This past week, the Novavax vaccine moved into Phase III clinical trials and along with two others manufactured by Johnson and Johnson and Sinopharm.
Another excellent vaccine development update from Nature:
https://www.nature.com/articles/d41586-020-01221-y
Vaccine allocation
When is it my turn to get this long-awaited vaccine?
Beyond the interest of this administration in politicizing the final approval and delivery of a Covid-19 shot, a vaccine is coming and will likely be approved by the end of the year if indeed the clinical trials are safe and effective as anticipated. Many of you want to know how long we have to wait before a vaccine materializes into a shot activating your immune systems and providing that protection we all crave.
This past week, the World Health Organization and the US National Academy of Sciences, Engineering and Medicine have proposed a five-phase plan to fairly allocate a coronavirus vaccine internationally and to US residents respectively. I invite you to read more about it here: https://www.who.int/publications/m/item/fair-allocation-mechanism-for-covid-19-vaccines-through-the-covax-facility and here: https://www.nap.edu/catalog/25914/discussion-draft-of-the-preliminary-framework-for-equitable-allocation-of-covid-19-vaccine
Debunking Myths: Q&A
1. Asymptomatic individuals do not transmit COVID-19. Myth!
Multiple studies indicate that nearly half of transmissions are from people not feeling ill! https://www.medrxiv.org/content/10.1101/2020.09.04.20188516v2
2. Do antibodies last and could I get re-infected with COVID-19? Myth!
The fact that after more than 6 million cases worldwide only one case was confirmed to have developed reinfection suggests to me that this is a very rare phenomenon. In late August, a 33-year-old Hong Kong resident, who had his initial infection in the early Spring, tested positive again upon return from Spain via the UK. He remained asymptomatic and mounted a vigorous antibody response to the second strain, confirmed by genetic analysis. Antibodies last several months and our cellular immunity takes over after antibody titers wane. https://www.nejm.org/doi/full/10.1056/NEJMoa2026116?query=featured_coronavirus
Antibody titers appear to remain elevated for 4-5 months after infection and then they start to decline. Gleaning information from the SARS-CoV1 epidemic of 2002, adequate titers of neutralizing antibodies remained elevated 2-3 years after acute infection.
3. COVID-19 is associated with increased risk of clotting and therefore we should take aspirin or blood thinners. Myth!
Patients who develop severe COVID-19 disease and usually those requiring ICU support, may go on to develop microthrombi and disseminated intravascular coagulation. For those patients, anticoagulation treatment is standard and decided by the ICU team at the time of care. Use of preventive blood thinners is unfounded!
4. Is the virus mutating to be able to be infectious through the skin?
No! there is no evidence that this is possible. The virus utilizes special receptors located in the respiratory epithelium called ACE-2 (Angiotensin Converting Enzyme type II) to be internalized and infect epithelial cells. Furthermore, the probability of becoming infected from packages and surfaces is extremely low. Stop wasting time and disinfecting surfaces and packages. Not likely to get to your upper airway in an adequate infectious dose.
5. Is the virus mutating such that development of an effective vaccine is in peril?
Of course, the virus is mutating, just like any other virus multiplying in the trillions and infecting millions of hosts, but there is no evidence that the minor mutations will lead to major changes in the antigens and virulence of the virus. SARS-CoV2 is a stable, non-segmented RNA virus and major mutations to alter immunogenicity and virulence during the course of the pandemic would be surprising.
6. UV light / silver and copper-based agents destroy SARS-CoV2 and are effective preventive or treatment modes. Myth!
While prolonged UV light may inactivate the virus, using UV light has no immediate effects and is potentially harmful. Metal-based products have no known effect on the virus
7. Do masks help decrease the severity of illness and could they diminish Influenza transmission?
Likely YES! There appears to be a relationship between the infectious dose and severity of illness. The rate of asymptomatic infection was estimated at 40% by the CDC in mid-July, but they have been reported to be > 80% with universal masking. In a closed Argentinian cruise ship outbreak, where all passengers and staff were provided with masks, the rate of asymptomatic infection was 81% (compared to 20% in earlier ship outbreaks). https://www.nejm.org/doi/full/10.1056/NEJMp2026913
Prevention!
Finally, allow me to repeat one more time that we should continue to support the World Health Organization (WHO)!
As of July 7th, 2020 the president of the United States, in his infinite “wisdom” and utilizing his unbounded “leadership” decided to withdraw the U.S. from the WHO. Those of you who have been following the news realize that this is just another stratagem to blame a defenseless organization for the dismal response from the White House and the executive branch of our government
The WHO is not perfect. It requires epidemiologic information from its member nations and needs invitations from those nations to carry out its work. It ensures drug safety and sets guidelines for treatments in nations that have more limited resources.
For a brief and insightful comment, read this: https://www.nejm.org/doi/full/10.1056/NEJMe2024894?query=featured_hom
Of course, humanity continues to witness so many preventable deaths and so much avoidable suffering. Yet, we have the tools to do better!
Think of the “malnutrition” afflicting the world. In most nations, obesity and its deadly complications. In a few, insufficient nutrition.
What about the constant gun violence in America? As the father of college children, who are fortunately healthy and enjoy science and the humanities, one of my main concerns is the random, indiscriminate and unpredictable fire-arm violence in our Nation. How could we not support back-ground checks and proper psychological testing and proficiency before we authorize purchase of guns? Most of us do not reside in the Wild West and the Second Amendment must be interpreted under historical context.
What about the “epidemic” of narcotic addiction and related mortality?
What about the “silent killer”: TOBACCO! It remains the leading preventable cause of death which dwarfs the COVID-19 mortality. Cigarettes kill ½ million Americans annually and many millions worldwide. The pandemic has claimed over 200,000 human lives to date in the US and 1 million worldwide.

Ozzy Covy Picone continues to defy the scale for over 100 lbs!
In the meantime, keep cool, do not panic, eat a nutritious and diverse diet, stay active and be happy!
Use a properly fitted mask while in public indoor places.
Take a multivitamin daily and don’t forget your 1000-2000 IU of vitamin D3.
Be ready to accept vaccination as soon as it becomes available. Likely by early 2021.
And let’s try to make the best lemonade with the “lemons” nature has thrown our way!
Fear is not a rational response. This too shall pass! Do not anguish about rare problems unless you have won the lottery more than once.
Remember that the only certainty in life is… death… (and TAXES, unless you are a famous shameless cheater rewarded with an important Public Servant job near you!) and the only fountain of youth proven by science, experience and millennia are exercise, laughter, humor and a good positive attitude!
Enjoy every minute of this most interesting JOURNEY and cherish this family time!!!
Carlos Picone, MD
5215 Loughboro Rd, Suite 400
Washington, DC 20016
301-656-7374
email: cpicone@chevychasepulmonary.com
References:
- https://www.nejm.org/coronavirus
- https://www.cdc.gov/coronavirus/2019-nCoV/index.html
- https://www.who.int
- https://clinicaltrials.gov/
- https://www.nature.com/articles/d41586-020-00154-w]
- https://en.wikipedia.org/wiki/Immune_system
- https://www.nejm.org/doi/full/10.1056/NEJMe2025111 https://www.nejm.org/doi/full/10.1056/NEJMe2024894?query=featured_home
- https://science.sciencemag.org/content/early/2020/05/12/science.abc5312 https://www.nejm.org/doi/full/10.1056/NEJMp2005630?query=featured_coronavirus https://www.youtube.com/watch?v=-Gn8oJY1VHY&feature=youtu.be https://www.cfr.org/backgrounder/what-world-doing-create-covid-19-vaccine
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3805090/
- https://www.nejm.org/doi/full/10.1056/NEJMcibr2009737?query=featured_coronavirus
- https://jamanetwork.com/journals/jama/fullarticle/2767840
- https://www.nature.com/articles/d41586-020-00502-w
- https://www.nap.edu/catalog/25914/discussion-draft-of-the-preliminary-framework-for-equitable-allocation-of-covid-19-vaccine
ANNEX: COVID-19 Timeline
From Nature:
https://www.nature.com/articles/d41586-020-00154-w
- 21 December, 2019, a few patients became ill with severe pneumonia in Wuhan, Hubei province of China.
- 31 December, 2019, a new virus is identified in samples from 4 patients with pneumonia of unknown cause. All patients had been present at the Huanan Seafood Market in Wuhan. Viral genome isolated and sequenced. Initially named 2019-NCoV (Novel Coronavirus 2019).
- 8 January, 2020 – Nature reports on the new virus, cause of mysterious “deadly pneumonia” in Wuhan, China.
- 21 January, 2020 – First US case confirmed in Washington State. 30 yo man returning from Wuhan, China.
- 23 January, 2020 – China closes Wuhan.
- 24 January, 2020 – Second US case. 60 yo woman returning to Chicago after visiting China.
- 28 January, 2020 – Human-to-human transmission confirmed in Germany.
- 3 February, 2020 – Study of live virus published.
- 6 February, 2020 – Retrospective autopsies completed in mid-April in Santa Clara, CA confirms that first deaths occurred in early Feb.
- 14 February, 2020 – Chinese authorities reveal number of infections in medical staff: 1,716 health workers had contracted the virus, 6 of whom died
- 17 February, 2020 – First case in Africa
- 25 February, 2020 – U.S. emergency funding for coronavirus response
- 26 February, 2020 – Brazil reports first case in South America
- 28 February, 2020 – Coronavirus spreads to sub-Saharan Africa
- 4 March, 2020 – Multiple drugs under investigation for coronavirus
- 5 March, 2020 – China study suggests children are as likely to be infected as adults, but most do not become ill.
- 11 March, 2020 – Transgenic animals for CV research in high demand
- 11 March, 2020 – Coronavirus becomes a pandemic, says WHO.
- 13 March, 2020 – US President declares “national emergency”. It is no longer a “Chinese virus that will blow over by the spring”.
- 17 March, 2020 – First vaccine clinical trials begin in U.S. (National Institute of Allergy and Infectious Diseases (NIAID) and Moderna (biotechnology company in Cambridge, MA) – “launched in record speed,” 66 days from genetic sequencing of virus to the first human injection of the vaccine candidate.
- 18 March, 2020 – Deaths in Italy surpass those in China.
- 19 March, 2020 – No new cases confirmed in Hubei, China.
- 25 March, 2020 – Retrospective studies in Lombardy confirm that the virus was present in Northern Italy in early January 2020.
- 1 April, 2020 – Over 80% of ICU patients with COVID-19 have underlying medical conditions.
- 2 April, 2020 – Worldwide cases surpass 1,000,000.
- 7 April, 2020 – No new reported COVID-19 deaths in China
- 8 April, 2020 – Tracking App reveals lack of smell is key symptom.
- 15 April, 2020 – Trump – in his infinite wisdom and trust-worthy scientific knowledge – suspends WHO funding. Leonardo Da Vinci’s birthday celebrated by “scapegoating” the WHO.
- 15 April, 2020 – Worldwide infections surpass 2,000,000.
- 21 April, 2020 – Mars probe HOPE ships from UAE to Japan for launch after July 15th when Mars and Earth are aligned. It should reach the Red Planet by 2021.
- 21 April, 2020 – https://1daysooner.org/volunteer 15,000 people volunteer to be exposed to virus and accelerate vaccine development.
- 27 April, 2020 – The five ways Trump is undermining environmental protection under the cover of the Pandemic: https://www.nature.com/articles/d41586-020-01261-4
- 29 April, 2020 – Remdesivir speeds up recovery!
- 7 May, 2020 – First CRISPR testing kit approved in US. It works by programming the CRISPR machinery to detect snippets of the virus genetic material and expedites results to 1 hour.
- 15 July, 2020 – Only medications with proven efficacy so far: Remdesivir (antiviral) and dexamethasone, when used in patients with pneumonitis seems to expedite recovery, but not early on. In fact, it may worsen outcomes when used at the outset of disease. Non-Invasive oxygen delivery may be associated with better outcomes.
- 16 July, 2020 – mRNA vaccine able to generate adequate immunogenic responses and phase III clinical trial to begin soon.
- 20 July, 2020 – Recombinant Adenovirus vaccine that encodes SARS-CoV2 Spike protein is highly immunogenic on phase I/II clinical trials conducted in the UK and phase III trials to start soon.
- 27 September, 2020 – Over 33,000,000 cases and almost 1,000,000 deaths worldwide. Over 7,000,000 cases in the US and 205,000 deaths. Pandemic tracker: https://coronavirus.jhu.edu/map.html
Download a PDF of this article
About SignatureMD
SignatureMD is one of the nation’s largest firms providing initial conversion and ongoing support services to concierge medicine physicians. SignatureMD currently partners with over 200 affiliated primary care physicians and specialists across 35 states, and its network is rapidly expanding.